|
There are many things about living on the mission field that can influence the physical health of missionaries and their families. The climate and conditions in the host country may be a shock to the physical body. The doubled impact of long-term culture and ministry stress may weaken the body’s immune system and make it more vulnerable to breakdown. When sickness does strike, the quality of health care in the host country may be questionable or inadequate. In host countries where infrastructure is lacking and “life is cheaper,” accidents and injuries can strike at any time. And we must never forget the factor of spiritual warfare: the enemy will do all he can to disable us, and that includes attacks on our health. When the body does not cooperate, even the most simple of tasks can become difficult. Mustering the energy to do the hard work of ministry and life overseas can become exceedingly difficult. Sickness can necessitate trips to the home country for treatment, or even permanent relocation to an area where full recovery is possible. We measured the frequency and strength of influence on the return decision for the following statements considered to be host-country-related factors:
A focus of this survey has been identifying areas of preventable attrition so that we may improve the experience of missionaries and lower attrition rates. When it comes to health matters, neither missionaries nor their sending churches and agencies are necessarily in control of how their bodies will respond to physical conditions, challenges, and illness. Country factors impacting health, such as climate and pollution, can hardly be changed. However, it is hoped that this data will be helpful for its descriptive value, as well as for the limited conclusions we can draw about preventable factors of attrition related to health. It may also suggest areas for deeper etiological research into the health of missionaries. Results The table below summarizes the results for each question by providing:
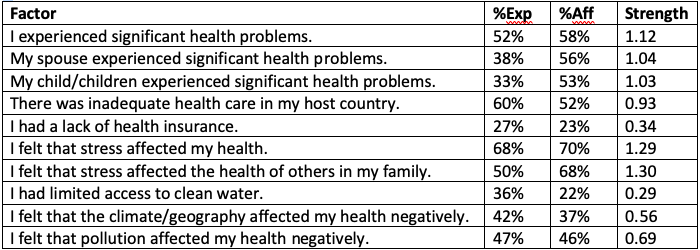 Discussion of Quantitative Results It is noteworthy that more than half of missionaries reported having serious health problems. More than one-third reported serious health problems for their spouse. And one-third reported serious health problems for at least one child. These are very high rates of sickness for the periods of time being reported (the average tenure was approximately 8 1/2 years). In all three cases, over half of the respondents reported that this issue affected their decision to return to their home country, and to an overall moderate degree. It is hard to know how much overlap there is between the three categories, but clearly many families have multiple people experiencing significant health problems, which can compound the stress of dealing with them. Sixty percent reported that health care was inadequate in their host country and 52% said that this affected their decision to return to their home country, also to an overall moderate degree. As people who may have the option to seek better health care in another country, it makes sense to do so for many missionaries with serious health problems. Certain treatments or expertise may not be available in the host country, may be at a great distance from where the missionary lives, or may be of lower quality given the limited resources of many developing countries for health care. Fortunately, most missionaries had adequate health insurance to address their health issues, even if they had to travel to another country to get the care that they needed. However, one-fourth reported that they either didn’t have health insurance at all or didn’t have the coverage that they needed. This affected the return decision of nearly one-fourth of those, though to a slight degree. The most significant finding of this section (and indeed, one of the most significant in the survey) is the degree to which participants felt that stress affected both their health and the health of their families. More than two-thirds felt that stress affected their health, while half felt that stress affected the health of other family members. In both scenarios, this affected the return decision in 68-70% of cases, and to a relatively strong degree. These findings seem to indicate that the whole family experiences the stress of living on the mission field and is affected by it. Spouses and children are not immune. In addition, when stress is affecting the health of the whole family, the likelihood of attrition greatly increases, perhaps because the family sees no way to reduce the stress other than leaving the situation. As access to clean water has increased worldwide, so has access for missionaries living in these areas. One-third of missionaries reported that their access to clean water was limited, but few of those (22%) reported that it affected their return decision, and to a low degree. Those in these areas likely knew this was an issue before arriving, came prepared to deal with it, and did not feel that it was debilitating enough to strongly affect their return deliberations, though it was certainly an inconvenience. Climate difficulties and pollution were reported by just under half of the respondents as affecting health, and in 37% and 46% of these cases, respectively, affected the return decision, but only to a slight degree. People reported in the open response section that air contamination, heat, and humidity (and the accompanying mold) affected them because they were not used to them in their home country. While inconvenient, it was not a strong reason for leaving for most. For those who did feel very affected in their bodies by these environmental factors, however, the only solution for improving health would be to leave the area, since these are not issues that can be changed. Qualitative Data To survey the most frequent types of health problems experienced by missionaries, in addition to the quantitative scaled data, we collected open comments on the following question:
We received 396 comments covering everything alphabetically from acid reflux to Zika. Problems reported were as manageable as intestinal parasites, and as catastrophic as the loss of a spouse or child. The collective pain reported truly shows the sobering costs of the missions call, and the astonishing bravery and stamina of missionaries in facing them. Many missionaries reported here on mental health issues that they and their families experienced. There is a subsequent section specifically pertaining to mental health, but at this point in the survey, respondents would not have known this, so some provided it here. One shared about a pollution-related sickness that had persisted 6 years after their return, but also commented that in even comparison to that, “the psychological/emotional/spiritual price to pay for the years we spent there were maybe more significant than just the physical (although I doubt they are unrelated).” The analysis of and commentary on mental-health-related data will be set aside until publishing of the relevant section, except for one very important observation: Missionaries reported mental health issues more than any physical health category, and this occurred without them being asked to include such issues specifically. To illustrate, the mental health data is included here for comparison only. The following table lists the most common major categories and the number of cases in reported in each: 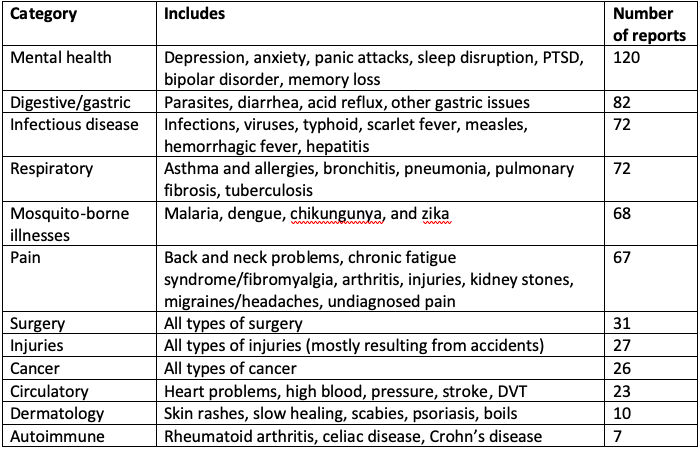 We must remember that these were self-reported “serious health problems.” We did not ask specifically about each possible health problem, nor define what constituted a serious health problem. Therefore, issues like parasites, asthma, and infections, for example, were likely under-reported because some participants did not judge those as sufficiently “serious” to warrant inclusion. The ones that were reported were likely more serious cases that caused greater complications. However, even taking into account potential under-reporting in some other categories, one cannot ignore the primacy of mental health issues on the mission field. One note of caution before drawing conclusions about the mental health of missionaries in general: This finding does not mean that missionaries experience greater rates of mental health problems than the general population, only that it is the greatest problem reported by missionaries. Any of the following three reasons could apply, or a combination of them:
It would be the job of medical professionals to establish whether missionaries experience higher rates of certain diseases than the general population, and what factors may contribute to their rates of sickness. Such conclusions are beyond the scope of this study. But perhaps this study can indicate further areas of research into the physical and mental health of missionaries. The following table lists, in descending order, the number of cases reported for each type of specific ailment mentioned in the comments, for those who would like a more detailed breakdown: 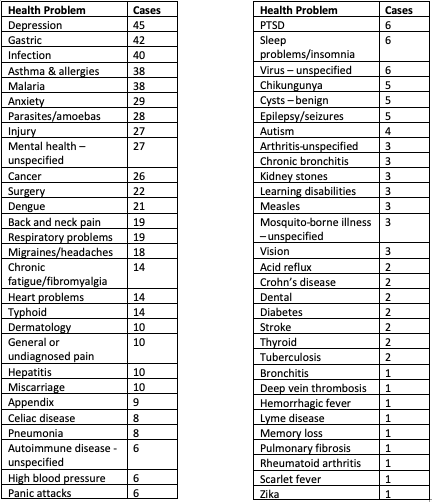 STRESS AS A CONTRIBUTING FACTOR
Another important observation is the role that stress can play in many of these physical ailments, either giving disease a foothold or exacerbating a problem that would otherwise be less severe. In fact, 52 commenters specifically mentioned that they believed or were told that their physical health problems were caused by high stress:
One participant shared that she and her husband were part of “an organizational culture of doing above and beyond what any one person can naturally do,” a common feature of mission culture, as we saw in the family factors section of this report where we discussed the issue of work-life balance. Her husband “leaned toward workaholic tendencies,” buying into the organizational culture. As a result, she felt that “stress levels at times greatly affected our whole family.” Another responder saw a relationship between their health and their ability to manage stress, saying “my ability to manage my stress in healthy ways gradually deteriorated over the years,” as did his/her health. Others commented: “I had to go to the hospital when I was having chest pains. My blood pressure was 240/139. Stress was the culprit.” “Stress played a huge role in my health. I did not necessarily come back because of health issues… but once I came back, I realized how much stress had affected every area of my life and health.” “Coupled with stress and constantly fighting malaria and taking lots of treatments, my immune system couldn’t fight off the malaria very well eventually.” One person was diagnosed in their second year on the field with an unspecified autoimmune disorder causing extreme joint pain and severe insomnia: “I learned that one of the primary causes of what I was experiencing was extremely high levels of cortisol from too much stress. Although I didn’t feel I was under that much stress on the field, my body said otherwise. Now almost three years after leaving the field, my hormone levels are finally starting to normalize and I am finally feeling healthy more days than not.” It is also important to recognize that the causality between stress and physical health (or mental and physical health) is not one-way. Physical problems cause stress as much as stress causes physical problems, creating a feedback loop that can create a downward spiral in both physical and mental health. “The main reason I left the field was because of depression and anxiety that became so serious that it caused other health issues, including respiratory problems, anxiety attacks, weight loss and gain, and a significantly weakened immune system.” ENVIRONMENT AS A CONTRIBUTING FACTOR Sometimes the physical environment in the host country was not conducive to maintaining the health of the missionaries and/or their family. This included primarily air pollution, but also natural substances that caused allergies or severe reactions. These comments illustrate how some places of service made people physically ill: “The pollution really affected my health and fibromyalgia. I struggled with sinusitis because of the pollution and my eldest had flare ups in his allergies due to the pollution. He sounded like he was sick all the time during peak pollution.” “My husband and youngest son are both asthmatic. We had to move house one time to get away from neighbors burning rubbish. Air quality in the capital city was really poor and affected them both.” “I developed severe respiratory problems in our second placement and several of my children had milder but similar symptoms. We are fairly sure these were caused by the extreme air pollution. Still not fully recovered almost a year later.” “My eyes got so bad with pollution that I couldn’t wear contacts any longer. I was sick a lot (intestinal and sinus). I also began to worry more about my children’s health/lungs raising them in such a polluted area.” “I began having severe migraines, nerve pain, numbing and skin trouble on my hands. This only happened when we were in our tribal location and began almost immediately. It led to times of bedrest and almost constant pain. After a few years and many medical visits, the doctors’ best guess was that it was the environment we served in as it was in a swamp and our house had a great deal of black mold that was impossible to get rid of. My husband later began to experience numbing as well. He also has struggled for many years with fatigue and this was worsened in this hot environment and high stress environment.” MENTAL AND PHYSICAL “GRIT” Reading the stories of health trials reveals one type of high price paid by some missionaries for their commitment to the call. The mental and physical toughness of these missionaries is also apparent. Far from being “weak” or debilitated by their health struggles, they were more typically strong individuals who stubbornly persisted for some time despite them. People were hospitalized repeatedly. “I went to my host country knowing I had Crohn’s disease, but my condition was stable. Throughout my 2 ½ years there, I was hospitalized several times. I underwent emergency surgery in the third-world country and was dying. I returned to my home country for medical help.” They contracted rare and “exotic” diseases that their home-country friends and family have probably never even heard about. “Two of our daughters contracted Chagas disease while serving in the jungle.” “Right after returning to Zambia for my second term, I was diagnosed with bilharzia and experienced severe joint pain and fatigue. Thankfully, I was diagnosed pretty much right away and felt relief!” More than a few faced near-death situations. “Had malaria 10 times in 6 years, twice life-threatening.” “A severe asthma attack in our 8-month old nearly took his life.” “One of our daughters became anorexic and came close to dying. She spent two months in a hospital in the U.S. Our second daughter was diagnosed with OCD.” Some “battled constant sickness” and “wondered if I would ever get better.” One participant shared of their family, “it seemed someone was always sick for three years.” “We were continually sick for long periods of time. My wife experienced burn out. My youngest son had a constant illness that wasn’t diagnosed until we went to a different country. He lost significant weight. I was diagnosed with cancer upon return to Australia.” “Multiple cases of malaria, hepatitis, dengue fever, skin rashes, diarrhea, fungal infections, scabies, intestinal worms etc., plus a work-related accident that tore muscles in my chest (6 months recovery) and a broken ankle (motorcycle accident).” “I had ongoing stomach issues and anxiety, husband had recurring amoebas, kids both had pneumonia and one had amoebas four times in a year, husband and I both had dengue fever.” Some health issues lasted for very long periods of time, affecting family and ministry life, and missionaries had to evaluate whether to stay or go “home.” “I contracted hepatitis A while I was overseas … that took about a year to recover.” “I had an illness that lasted 3 years that slowed my ministry down to almost nothing. Then I was healed and began ministry again.” “My husband was diagnosed with cancer after we left the field that should have been diagnosed on the field. We both felt exhausted even after a six-month sabbatical (which really wasn’t a rest as we used the time to do fundraising). We tried to practice good self-care. My husband’s cancer caused fatigue which we blamed on stress and living conditions instead of looking for a medical answer. My husband died two years after we left the field, at age 63, as a result of his cancer.” Many had to return for access to the kind of medical care that they needed, while others were able to receive care in their host country. “Baby born in country, had cancer at 8 months, home for chemo, return to country, war broke out, home again, stayed home because of side effects of chemo and learning needs.” “Was hypoglycemic due to diet, stress, and the way I responded to both by overproducing insulin leading to pancreatic and adrenal disorder. A fellow missionary doc told me to return home or I’d die in 12-18 months after viewing my test results. He prayed that maybe someone in the U.S. could find out what caused me to lose 50 pounds in 5 weeks. Returned to U.S. and 5 months later had a triple bypass.” “Miscarriage and my first ever hospitalization, our toddler son had croup and had to be hospitalized, I had hepatitis A, we all had various parasites, I was diagnosed with breast cancer. Our family returned to the U.S. for 8 months, then returned to the field for one more year before we left for good.” Some health issues cleared up once missionaries were in the home country, but others suffered lifelong health effects. “Malaria a few times was pretty easy, but 18 months of a staph infection, complete with boils covering my torso, became a problem. The 14 rounds of antibiotics started a chain of digestive issues that are still a problem 15 years later.” Some withstood a barrage of health crises, or a sudden decline, in a very short period of time. “In one three-month span, had appendicitis, measles, chikungunya, and shingles.” “I lost 18% of my body weight in one month due to gastrointestinal issues.” “Serious motorcycle accident with knee damage, a dog attack requiring facial reconstruction, a severe concussion, a broken arm requiring surgery… and much more, and we were only there for 18 months!” “Upon arrival to Togo, I quickly began to experience debilitating migraines that lasted up to a week. This occurred at least once per month.” The children of missionaries are not exempt from physical and emotional suffering. Parents find it particularly difficult to watch their children’s health suffer, especially if they feel that it may be related to their own lifestyle choices. “The children had malaria repeatedly.” “My child almost died from a sudden illness, and the top doctors/hospitals in the country indicated they could do nothing for us. My daughter was allergic to all the antibiotics they had. They said they had no more available. Doctors told us that ‘if’ she survived, it could happen again, and this country simply could not help her.” “Both of our teens had depression.” “One child suffered from severe anxiety together with failure to thrive, another suffered from chronic stomach aches/reflux but no underlying medical cause was found despite extensive testing.” In many of these stories, any one of the issues would have been the cause of great suffering. Chronic pain, respiratory problems, or gastric issues are difficult enough to deal with on their own. But when other issues get layered on, such as parasites, infection, surgery, or mental health issues, it can become very hard to function. When more than one person in the family is sick, the effect is multiplied and one can feel that all time is spent trying to get people healthy again. Having a health emergency is frightening enough in one’s home country. Being in a place where you are not sure you can even get the medical care that you or your children need can cause an entirely different level of anxiety and uncertainty. One participant shared, “Frankly, any health issue seemed to be serious in an overseas context.” This is a sense of vulnerability that people in the home country cannot often understand. It is truly impressive how much missionaries are willing to endure for the privilege of participating in the Great Commission. Sending agencies, churches, and friends back home should be aware of what missionaries may go through physically in order to provide the necessary emotional and practical support when health problems strike. LACK OF SUPPORT AS A CONTRIBUTING FACTOR Even when faced with severe physical or emotional challenges, some said that they still would have stayed were it not for other barriers that came into play. For some, it was a lack of team support during health trials. One woman shared that team members expressed relief after her miscarriage, because they had not wanted the burden of having to help with an unplanned pregnancy and a new baby. Another had a young child nearly die because of her inability to absorb antimalarials and was subjected to “criticism and hurtful comments” by their home community that: “we must have been in ‘sin’ or God wouldn’t have allowed our daughter to get so critically ill with malaria. Some criticized us and said that we should have used medicine rather than relying on our faith, as they had never heard of a child not responding to antimalarials or malarial treatments. A few said if we had been called to the mission field, we should have stayed even if our daughter had died out there.” Some felt they could have stayed with minimal support from their team. Far from home and without a community who would draw around them during difficult times, these missionaries ended up heading back to the home country where a stronger support network awaited them. “The leaders of the mission were unwilling to help me secure the medicine I needed to stay. Instead, they opted to send me home when all I really needed was an inhaled steroid.” Some commenters even felt that their physical symptoms were the result of stress related to team dynamics. “My husband started experiencing serious headaches and had to leave for further evaluation. From what we know now, those headaches were due to the immense stress of living on such an unhealthy team.” This was not the only person to comment on how team conflict created a stressful environment that affected their health. It’s a good example of crossover between factor categories, in this case between team factors and health factors. No factor operates in isolation from the others in a missionary’s life. They constantly interact to form a complex web of cause-and-effect relationships. Conclusions What can we learn from this data to help us better serve our missionaries? How can missionaries best protect themselves from health dangers on the mission field? Physical health is important to all people everywhere. It enables us to have the energy and ability to follow our dreams and calling. When the body is working well, we don’t think about it. When it malfunctions, restoring it can quickly become the focus of our concern. Poor health can hobble our ministry as quickly as team conflict, family emergencies, or a loss of funding. We must not idolize physical health, for we know that our bodies are subject to decay and that God works through suffering as much as (or more than!) He does through health. But neither must we ignore it, naïvely missing its importance to our ability to serve. With this model of being good stewards of our missionaries’ health, but also recognizing that we are not in full control of it, we can do the following things.
And when sickness does come, we can remember that this too is forming us into Christ’s image. God still loves and cares for us even when He allows us to pass through difficult times, and these same trials can be used to glorify Him. Therefore, since Christ suffered in his body, arm yourselves also with the same attitude, because whoever suffers in the body is done with sin. As a result, they do not live the rest of their earthly lives for evil human desires, but rather for the will of God. 1 Peter 4:1-2
1 Comment
|
